Kidney Stones, or ‘renal calculi’ are a very common urological condition, affecting up to one in eleven people, causing severe and sudden attacks of pain, and in some cases, serious infection or kidney injury.
 Stones arise when naturally occuring, dissolved substances in the urine come together and form solid ‘crystals” in the kidney. These microscopic crystals then attract other particles in the urine until a stone or ‘calculus’ is formed.
Stones arise when naturally occuring, dissolved substances in the urine come together and form solid ‘crystals” in the kidney. These microscopic crystals then attract other particles in the urine until a stone or ‘calculus’ is formed.
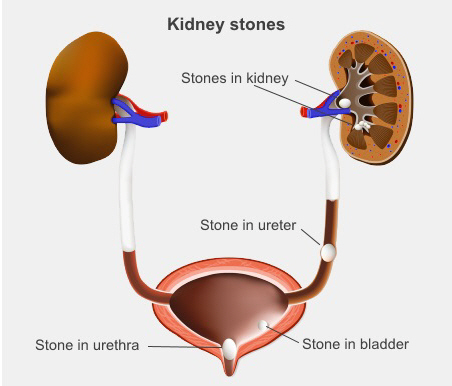
Most stones within the kidneys don’t cause any pain. However, if a stone falls out of the kidney and blocks the ureter, the very narrow tube that runs from the kidney to the bladder, the sudden blockage results in extremely severe pain, often associated with nausea and vomiting. This pain is known as ‘renal or ureteric colic’, and most sufferers end up in an Emergency department requiring very strong pain relief. Other symptoms of stones may include pain in the groin, or testicles in men, needing to go to pass urine more urgently, or some blood in the urine.
Stones are diagnosed by an imaging test called a CT KUB. Many smaller stones (less than 4-5mm in size) may pass out of the urinary tract but this can often take a number of days or weeks and some may cause ongoing pain. In general, if you have an attack of pain caused by a small stone, your pain settles, and you are otherwise well, it’s safe to undergo a ‘period of observation’ to see if your stone passes. However, you should make sure that you have another CT KUB scan after 4-6 weeks to see if the stone has gone, even if you do not have any further pain. It is also important to follow up with your local doctor, or your specialist with your CT scan.
Most kidney stones contain calcium, and the majority of these stones are made of a substance called calcium oxalate. Although some people with calcium stones may have higher levels of calcium in their urine, many stone-formers actually have normal amounts calcium in their urine. A common myth is that consuming a lot of dairy products or taking calcium supplements causes calcium stones. Calcium is an important part of a healthy diet, and restricting calcium intake too much can actually result in more kidney stones forming.
Other types of kidney stones are:
- Uric acid stones. Uric acid is a waste product of metabolism and is cleared from the body through the urine. Some people produce more uric acid than normal, and can form uric acid stones. Uric acid stones cause the same symptoms as calcium stones, and some individuals will form ‘mixed’ stones, which are composed of uric acid and calcium oxalate. In people who repeatedly develop uric acid stones, medications which reduce uric acid excretion or decrease the acidity of urine (pH) can be beneficial in stone prevention.
- Struvite/infection stones. These stones occur in people who have chronic or repeated urinary tract infections caused by particular bacteria. These bacteria find their way into the kidneys and cause chemical changes in the urine which allow stone to form around the bacteria. They are much less common than calcium or uric acid stones, but are more difficult to treat effectively, because they are often very large, and irregular in shape. These stones are often referred to as ‘staghorn’ stones, because they form a cast of the inside of the kidney.
- Cystine stones. Cystinuria is a rare, inherited metabolic disorder where high amounts of of a substance called cystine persist in the urine, causing stones to form. People with this condition may form literally hundreds of stones through their lifetime, and almost always have a know family history of the condition.
In most people with kidney stones, there is no indentifiable cause, as stone formation occurs due to the individual properties of urine, as well as anatomical variations in a person’s kidneys. This is propbably why there is often a family history of stone formation. In addition, despite the many anecdotal remedies that patients report (eg. apple cider vinegar, boiled parsley, medicinal teas, beer) there is no way to definitely make a kidney stone pass or to prevent stones from recurring.
Management options for kidney or ureteric stones are:
- Ureteric stenting, involves placing a long thin tube passing from the kidney, down the ureter into the bladder. Stenting does not get rid of a kidney stone, but is a very common emergnecy procedure performed to relieve blockage caused by a stone in the ureter. If a patient has a stent placed, they will need to return to hospital at a later date to have their stent removed and the stone treated. Ureteric stents are also placed after stone treatment (see URS below) to prevent kidney blockage and to help stone fragments to pass.
- Shock wave lithotripsy (SWL), uses powerful soundwaves generated from outside the body to treat stones in the kidney and ureter. This is the ‘least invasive’ form of stone treatment and is ideal for treating small kidney stones, to prevent future attacks of stone pain. The shock waves are focused on the stone under X-ray guidance, with the aim of breaking the stone into very small pieces that can wash out of the kidney over a period of weeks. It is performed as day surgery, and there is usually minimal postoperative pain or discomfort. Dr Patel is one of the most experienced practitioners of SWL in Australia.
- Ureteroscopy (URS) and laser, is used to treat stones in the kidney and ureter. It involves passing a very small long scope, called a ureteroscope, into the bladder and then up the ureter and into the kidney, so it uses the the natural channels in the urinary tract. The stone is located under direct vision, it is broken up using very safe and precise laser energy through the scope. It is the most common way in which stones are treated, and is usually highly successful. It is suitable for treating larger stones, up to 2.5cm in size, anywhere in the kidney or ureter. Most patients who undergo URS require a temporary urinary stenting to help drainage of the kidney after treatment.
- Percutaneous nephrolithotomy is used to treat large stones in the kidney. The procedure involves making an incision in the back or side, to allow a rigid instrument called a nephroscope to be passed into the hollow center part of the kidney where the stone is located. An instrument passed through the nephroscope breaks up the stone and suctions out the pieces.
As mentioned, kidney stones can’t completely be prevented, but it is important for patients, particularly repeated stone-formers, to undergo testing to see if there is any way to potentially decrease their risk of stone formation. Once you have had your stone(s) successfully treated, Dr Patel can arrange specific blood and urine tests to see if there is any abnormality that can be treated. In addition, retrieved stone fragments can be sent for biochemical analysis to clarify what kind of stones an individual is forming.
Although one’s diet doesn’t usually play a major part in causing stones to form, certain dietary advice may have an impact on preventing stone formation. For example, patients with calcium stones may benefit from reducing their daily salt intake.
It is also believed that patients at risk of forming kidney stones should maintain a good fluid intake at all times. This is particularly important in the warmer months of the year, when people tend to lose more fluid through perspiration or what is termed ‘insensible fluid loss’. As a general rule, stone formers should drink enough to keep their urine as pale in colour as possible, and aim for a daily urine output of 2-2.5 litres over a 24 hour period (they can mesure this themselves).
Various medications may be prescribed for repeat stone formers, depending on the type of stones they form, to try to reduce their risk of further stone formation.
For many people, kidney stones are a chronic condition, so it is important to consider the above advice as long term measures that may help to prevent stone formation. In addition, since most stones only cause symptoms when they suddenly fall out of the kidney, patients need to have their kidneys monitored at periodic intervals with CT KUB to see if they are forming new stones. It is always preferable to treat kidney stones before they cause a severe attack of pain.