Kidney, or renal cancer, is the tenth most common cancer in Australia. The most common type of kidney cancer is called renal call carcinoma (RCC)
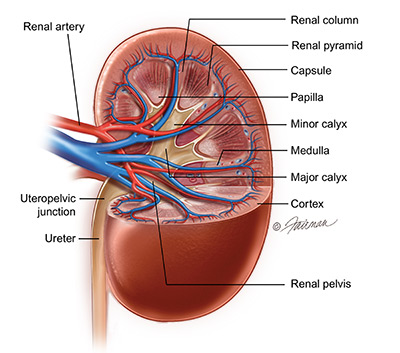 There are two main areas in which kidney cancers can arise. The renal parenchyma is the solid outer part of the kidney, and it contains millions of microscopic structures called nephrons which filter waste products from the bloodstream, and help to maintain the chemical balance in your body. The central part of the kidney is the pelvicalyceal system which is the hollow part into which urine filters from the nephrons, before it flows down the ureter into the urinary bladder. Cancers that arise from the cells of the renal parenchyma are called renal cell carcinoma (RCC) whereas tumors that arise from the lining of the pelvicalyceal system are called urothelial tumors.
There are two main areas in which kidney cancers can arise. The renal parenchyma is the solid outer part of the kidney, and it contains millions of microscopic structures called nephrons which filter waste products from the bloodstream, and help to maintain the chemical balance in your body. The central part of the kidney is the pelvicalyceal system which is the hollow part into which urine filters from the nephrons, before it flows down the ureter into the urinary bladder. Cancers that arise from the cells of the renal parenchyma are called renal cell carcinoma (RCC) whereas tumors that arise from the lining of the pelvicalyceal system are called urothelial tumors.
Typical symptoms or signs of RCC are:
- blood in the urine (microscopic or macroscopic)
- loss of appetite or weight loss for no apparent reason
- anaemia and fatigue
- a lump in the abdomen – only if the tumour is very large
However, many kidney cancers nowadays are diagnosed unexpectedly, or incidentally, in people who have had an ultrasound or CT scan for other reasons such as urinary symptoms, abdominal pain, or back pain. These tumours are often detected when they are smaller, and not causing any symptoms.
In most cases of kidney cancer there is no obvious cause, however there are some known risk factors:
- smoking
- obesity
- uncontrolled high blood pressure
- known family history
- inherited conditions (von Hippel Lindau syndrome, tuberous sclerosis)
Kidney tumours, or solid growths in the kidney, may initially be picked up on ultrasound scan which shows a suspicious area in the renal parenchyma. However it is always necessary to have a ‘triple phase’ CT scan or an MRI scan of the kidneys to provide clearer and more accurate images of a possible cancer, and to the visualise the other structures and organs in the abdomen. In addition, core biopsy of a solid tumour in the kidney may be indicated in some cases, to confirm a definite diagnosis. While most solid tumours of the kidney are cancerous, there is one type of solid tumour that occasionally occurs, called an oncocytoma, which is non-cancerous, or benign.
There are several different types of RCC, but the most common is called clear cell carcinoma, and this form of RCC usually has a good chance of cure if it is found early. The size of a kidney cancer when it is diagnosed is the most important factor in determining the chances of it being cured with treatment. In general tumours which are 7 cm or less in size will have a higher chance of cure than larger tumours.
Treatment options for kidney tumours should take into account:
- the size of the tumour
- where in the kidney the tumour is located
- patient age
- general health of the patient
- patient preference if there is more than one treatment option
In elderly patients, or in patients with other serious health problems, it is sometimes preferable to monitor small cancers (less than 2-3cm across) with periodic scans, rather than proceed with definitive treatment. Small tumours usually have a very low risk of spreading, or metastasising, to other parts of the body. Cryotherapy or radiofrequency ablation (RFA) are two minimally invasive ways of treating small kidney cancers in selected cases. These treatments should only be considered after discussion with a urologist.
The most accepted curative treatment for kidney cancer is surgery. This usually involves removing the entire kidney (total nephrectomy) by laparoscopic or ‘keyhole” surgery. In some cases where the cancer is small and growing outwards from the kidney surface it may be possible to remove only the tumour and leave the remainder of the kidney behind. This is called partial nephrectomy or nephron-sparing surgery, and the main aim of this surgery is to preserve as much kidney function as possible. It is obviously particularly important in patients who have pre-existing kidney disease, or who have had one kidney removed previously . Partial nephrectomy is a much more complex procedure than removing the entire kidney and definitely has an higher complication rate than total nephrectomy.